Assessing and modifying light and noise levels in the environment can contribute to providing dignified care for older people with dementia and for other older people with a range of sensory and cognitive impairments.
In an environment where there is no education, audit or regular evaluation of noise and light levels, sensory stimulation can become unbalanced. There are many situations, in various care setting, where people with dementia exhibit what are often referred to as ‘behavioral problems’, such as anxiety and agitation that are partially a consequence of being in an environment that is not dementia friendly or enabling. At the core of this is often sensory overload or under load from noise and light sources.
Most care settings are noisy places. Older people would not be used to the levels of noise, the continuous noise and noise associated with movement going on around them in their own homes. Background noise from telephones and machines, trolleys and other pieces of equipment, the television and radios all increase auditory stimulation. The motion of people coming and going also adds another layer to auditory stimulation.
Noise levels in hospital can become a form of environmental pollution. Sudden noises, such as when equipment is dropped or when doors arc slammed, cause a startle reflex, which as well as causing various physiological responses in the person with dementia, can also increase their sense of disorientation and insecurity.
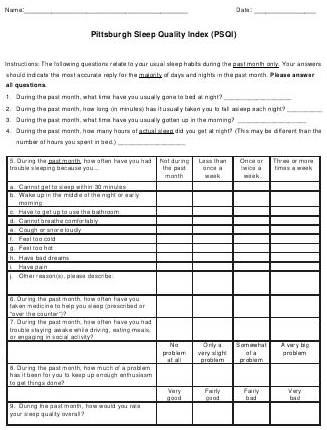
Assessment of noise and tight levels in the environment is the first step to providing a more person-centered and dementia-friendly environment.
- Typical Decibel (dB) Levels:
Threshold of acute hearing – 0 dB
Rustle of Leaves – 10 dB
Sleeping, studying, whispering – 30 dB
Conversation, comfort – 50-60 dB
Safety Threshold – 85 dB
Rock Band – 120 dB
Threshold of Pain – 130 dB